Magnetic-cap over Mini-implant Abutment

Applied in the U-shaped Maxillary Overdenture – Case Report
Chen, Tien-Kuan*, DDS
DDS, Kaohsiung Medical University, Taiwan
Chief, Roma Dental Clinic, Taichung Taiwan
Abstract::
Patients afraid of severe invasive implant surgery yet with less residual
maxillary natural teeth sometimes choose overdentures as a way of
rehabilitation and somehow magnetic abutments are considered as one way of
supporting elements for retention. If the abutments of natural teeth are
located ideally, an U-shaped maxillary denture base can be a comfortable
choice instead of the one that covers the palatal side. However, if the arch
is distally free end edentulous, the retention is going to be endangered and
the denture base inevitably has to cover more so the U-shaped one may be
given up. Mini-implants are generally less invasive due to small wounds,
less bleeding, no suturing, and being often painless after surgery so that
they are more acceptable for sensitive patients. But it is well known that
mini-implants are not so stable as normal implants under the long term bite
force. This one year followed case report is to demonstrate a design
invented by Dr. Tien-Kuan Chen, the reporter of this case, to help form an
U-shaped denture base for a distal edentulous maxilla. It is a simple
magnetic-cap cemented to the head of a mini-implant put at the distal free
end spot and serves as a magnetic abutment just as it is done by a natural
tooth. Magnetic abutments are usually made short to get less horizontal
forces, always as hazard forces, so that the abutments are less forced
mobile and their lives are longer. If the major function of a mini-implant
is merely as a magnetic abutment, it will gain the same benefits as well. In
comparison with the traditional big size implants for maxillary
rehabilitation, magnetic-cap over mini-implant abutments offer another
simple option in ways of shorter treatment time, longer abutment lives,
being less
invasive and more acceptable by sensitive patients.
Chief complaint & clinical examination
The patient, 59-year-old female, complains of being forceless and painful on
maxillary teeth as eating. She asks for the most non-invasive way to rebuild
her maxillary teeth and no coverage of her palate if a movable denture is
necessary. There is a long 14-units-in-one-piece porcelain crown-bridge with
abutments of #17, 13, 23, 25 and 27 on maxilla and all mobile (from GI to
GIII: #17- GIII, #13- GI, #23- GI, #25- GIII, #27- GII). From panoramic film
it shows bone absorption around all maxillary tooth roots more or less.




fig. 01:maxillary right molar root exposure
fig. 02: gum swelling at maxillary left posterior buccal side
fig. 03:maxillary occlusal view shows a long 14-units-in-one-piece porcelain
crown-bridge
fig. 04: The removed maxillary bridge shows severe inflammation around #17
(#27 crown is separated and still left inside the mouth for vertical
dimension taking. Later it will be cut short as well and transformed into a
magnetic abutment.)

fig. 05: pre-treatment panoramic film, taken in April. 21. 2005
Treatment plan
An U-shaped magnetic overdenture for maxilla with natural teeth (#13, 23,
25, 27) as magnetic abutments and a magnetic-cap over mini-implant abutment
put at the right distally edentulous site of maxilla itself
Treatment procedure (all in two weeks)




fig. 06: Natural teeth (#13, 23, 25, 27) as magnetic abutments and a
magnetic-cap over mini-implant abutment put at the right distally edentulous
site of maxilla (Implant is set at approximately the original site of #16,
but #17 is extracted meanwhile due to no bone support.)
fig. 07: the denture with magnets buried inside its tissue surface which
possesses magnetic retention
fig. 08: the U-shaped magnetic overdenture for maxilla, tissue surface view
fig. 09: the U-shaped magnetic overdenture for maxilla, occlusal surface
view




fig. 10: the U-shaped magnetic overdenture on maxilla
fig. 11: central occlusion, right side view
fig. 12: central occlusion,left side view
fig. 13: central occlusion, frontal view




fig. 14: natural smiling
fig. 15: natural big smiling
fig. 16: rest expression
fig. 17: laugh brightly
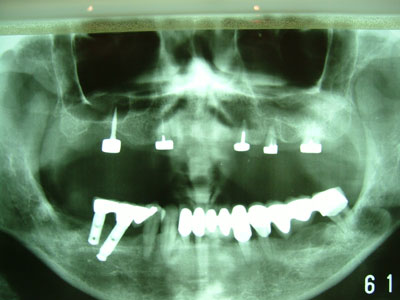
fig. 18: post-treatment panoramic film, taken in May. 5. 2005
Magnetic-cap over mini-implant abutment design & placement
(Fig.19-24 demonstrated are from the other patient.)



fig. 19: mini-implant with carved concave square head, 10 mm in length, 1.8
mm in diameter
fig. 20: mini-implant put inside maxillary alveolar bone directly and
photographed instantaneously; small wound, no suturing, and almost no
bleeding all the way
fig. 21: magnetic-cap, magnetic surface



fig. 22: magnetic-cap, cement surface with a major hole and multiple
smaller holes inside
fig. 23: filling cement into the cement hole of the magnetic-cap
fig. 24: magnetic-cap cemented to the head of the mini-implant put at
maxilla for immediate loading

fig. 25 : a widened chamber for the magnetic-cap in tissue surface of the
denture to avoid horizontal hazard force as eating
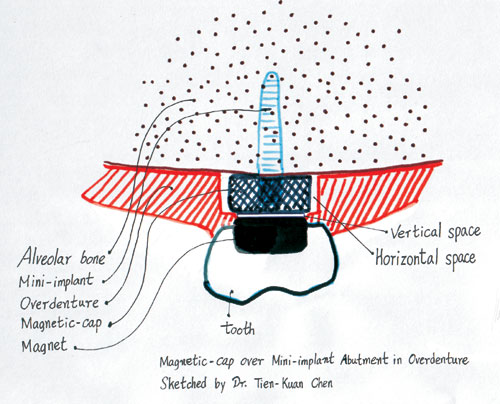
fig. 26: remove the adjacent resin a little bit around the magnetic-cap to
avoid horizontal hazard force as eating
After fourteen months from the delivery day
◎ Chief impression from the patient
Rather good in condition, easy to eat, the denture in stable position while
eating, satisfied of the appearance as talking and laughing, more convenient
to take care of oral hygiene then the
◎ Clinical examination



fig. 27: stable U-shaped maxillary denture in oral cavity
fig. 28:magnets in good shape
fig. 29: magnetic power check separately for every single magnet, all good



fig. 30: all magnetic-caps and roots in good condition, no inflammation and
no
mobility(except for #25 in GI mobility, but better then it was in GIII
mobility 14 months ago)
fig. 31: satisfied of the appearance by the patient as talking
fig. 32: satisfied of the appearance by the patient as laughing

fig. 33: The magnetic-cap of the mini-implant abutment gets well combined to
the gingiva of the ridge and no inflammation is found. In the past 14
months, it was just roughly brushed for 30 seconds two times a day by the
electrical tooth brush, and no dental flossing was done for itself.
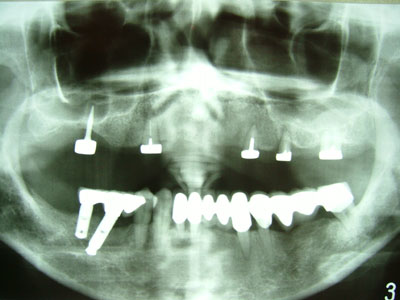
fig. 34: The panoramic film taken in Aug. 4. 2006 shows the bone around the
maxillary roots stops getting worse. Moreover, the bone around the
mini-implant is getting denser then it was 14 months ago (fig.18) which
indicates this mini-implant is going to have a stable future in the oral
cavity and ensures the U-shaped maxillary denture base can be maintained.
Discussion & Conclusion
1. An overdenture presses both on alveolar bone and residual roots. If
residual roots get reduced to keep a tiny space from the tissue surface of
the denture and also able to supply retention, the overdenture is going to
be steadier as eating and gets a longer life because the residual roots get
no harm from the occlusal force. Magnets can release their attractive power
to magnetic metals from distance and instantaneously not to be touched by
the metals themselves. A magnetic overdenture uses magnetic abutments for
retention and the abutments can be designed as no touch to the denture,
therefore better stability and a longer life are both gained
2. Mini-implants are now regularly applied in orthodontic treatment and
generally get good results. They provide long term maintained small forces
to shorten the treatment time yet seldom get themselves lost from oral
cavities. It shows generally the long time stand under small forces is
acceptable by alveolar bone even it is done by a mini-implant. In this case
report, the magnetic-cap over mini-implant abutment only executes the
magnetic power to the denture but gets fewer forces as eating. Horizontally,
the magnetic-cap chamber of the denture is widened (fig. 25 & 26) to avoid
the grinding force of eating, usually a hazard force. Vertically, the
magnetic-cap chamber base is reduced a very little bit (fig.35,36& 26) to
avoid sudden hard forces while chopping. In this way, there is no apparent
force to threaten the abutment and it will easily stay well in the oral
cavity for a long time.


fig.35: The vertical cushion between the magnet and magnetic-cap can be done
by a piece of tinfoil when a magnet is set into the denture.
fig.36: Then remove the tinfoil sticker from the magnet to create a cushion
space.
3. Traditionally, an implant needs time to get integration with bone around
so no early loading is helpful. This kind of long time waiting is not adored
by patients so immediate loading implant techniques are advanced but they
are also challenged by hard force damages in the early time after implant
surgeries. Magnetic-cap over mini-implant abutments, as the above-mentioned,
get little forces as biting so they integrate more easily with bone even
when they are loaded immediately by the magnetic power after being
implanted. This design, therefore, reduces the possibility of failure and
saves more time for patients.
4. Clinically, there are some sensitive patients who are afraid of or even
subjectively refuse invasive treatments. In some cases, the patients
complain of constantly dropping of their upper complete dentures as talking
because of gravity but actually it is due to severe absorption of the
alveolar ridges of complete maxillae. Magnetic-cap over mini-implant
abutments, under such circumstances, are more smoothly accepted by patients
themselves to help rebuild their maxillary occlusions according to small
wounds, no suturing, less bleeding, and being painless after surgeries in
comparison with normal big size implant ones. Furthermore, this design may
help form an U-shaped maxillary denture base in a fast and easy way for
patients who have less or even no teeth left. Consequently, suffering from
poor retention and less sense of taste due to the maxillary complete denture
with a big base are both no longer annoying problems.
References
1. Alfred H. Geering, Martin Kundert, Charles C. Kelsey. Complete Denture
and Overdenture Prosthetics. New York: Thieme, 1993.
2. George Graber, Urs Haensler, Peter Wiehl. Removable Partial Dentures. New
York: Thieme, 1988.
3. Minoru Ai, Yuh-Yuan Shiau. New Magnetic Application in Clinical
Dentistry. Tokyo: Quintessence, 2004.
4. Hiroshi Muraoka. A Compilation of Complete Denture Techniques. Tokyo:
Quintessence, 1989
5. K. H. & E. M. Rateitischak, H. F. Wolf, T. M. Hassell. Color Atlas of
Periodontology. New York: Thieme, 1985.
6. Kyoo-Ok Choi, Young-Kyun Kim, Hyun-Sik Park, Yong-Seok Cho, Tae-Gwan Eom.
2005 Osstem Implant System. Seoul: Osstem, 2005.